
Some people aren’t getting tested for COVID-19 because they don’t want to know if they have it.
Experts say that along with misinformation, the emotional and financial costs of contracting the pandemic disease could be driving some people to avoid the tests. Changing the way we talk about the pandemic could help address the problem.
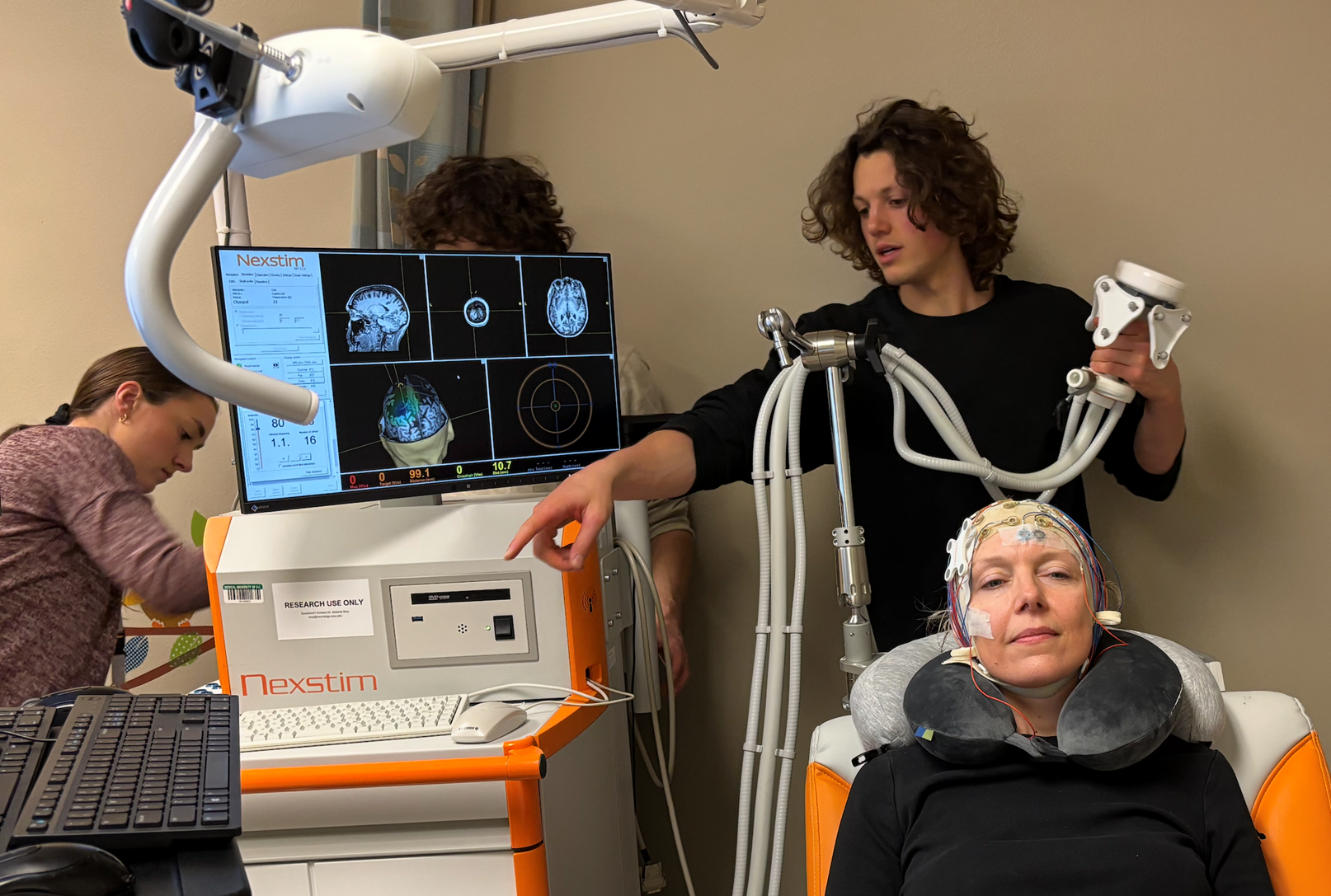
Data suggests not enough people in Wisconsin are being tested for the coronavirus.
News with a little more humanity
WPR’s “Wisconsin Today” newsletter keeps you connected to the state you love without feeling overwhelmed. No paywall. No agenda. No corporate filter.
Since November, Wisconsin has had a daily testing capacity of more than 59,000 tests, but supply has been outrunning demand. With the exception of Jan. 6, Wisconsin hasn’t cracked three-quarters of its testing capacity since Nov. 24, when the state was in the midst of a surge that was straining hospitals across the state.
Another indication is the state’s seven-day positivity rate per person, which tracks the average percentage of all people tested who test positive over the course of seven days. In Wisconsin, the rate started climbing into the 20-percent range in October and nearly approached 40 percent in November. As of Jan. 31, the rate was nearly 20 percent.
That’s too high, said Geoffrey Swain, founding director of the Wisconsin Center for Health Equity, a Milwaukee-based organization that looks at the social determinants of health, including how people’s economic circumstances affect their health decisions. Swain said that if enough people were being tested, the rate would be less than 5 percent.
“What it means is that probably only the most serious cases are getting a test, and not enough people who have mild cases are getting a test,” Swain said.
That makes it hard to control the spread of the disease, since it can be spread by people who have mild or asymptomatic cases.
This avoidance could be due to a number of factors: People may be feeling burnt out as the pandemic’s hold on the country closes in on the one-year mark, or they might not have access to testing.
But part of it could be more nuanced than that.
Testing positive means missing work, and for those without paid leave that means missing paychecks, too. It’s a strong disincentive to get tests, said Kathleen Murphy-Ende, a clinical psychologist at the University of Wisconsin Hospital and Clinics’ Department of Psychiatry. Patients have brought this up in her practice.
“People don’t have the sick leave, perhaps. Maybe they can’t take the time off work,” Murphy-Ende said. “Sometimes I think we underestimate the impact of finances on people’s behaviors with COVID.”
The Journal of the American Medical Association wrote in its November issue that test avoidance appears to be a growing problem. Some believe it’s their right to not get tested. Others feel anxiety about having to quarantine and isolate if they do test positive. The JAMA article points to groups of people in Utah refusing to get tested so that their schools wouldn’t shut down.
In these cases, Murphy-Ende said brushing off one’s own symptoms as something other than COVID-19 can feel less burdensome — a feeling, she said, her patients have discussed with her.
“Several people have expressed their worry about the impact if they’re positive on their close contacts,” Murphy-Ende said. “One person shared with me feeling guilty about having been in an unsafe situation in a restaurant, and then ended up with COVID. I think avoidance is something that people use as a coping mechanism.”
The public conversation about COVID-19 may be partially to blame for the reticence to test, said Julia Marcus, an infectious disease epidemiologist at Harvard Medical School.
She said that people often hear messages from public officials — and many others — like, “this is not hard,” “stop whining,” “don’t be selfish” and “don’t be reckless.” This can do more harm than good.
“My concern is that when people do test positive, then they immediately feel like, ‘Oh, I must have been irresponsible,’” Marcus said.
Rather than changing behaviors, shaming people for breaking safety protocols can make people defensive and resistant to taking public health advice.
“You need to respond to that by making sure that people have the tools they need to protect themselves if they do take risks,” she said, “because clearly some people are going to.”
Marcus said that simply prohibiting social interactions can be analogized to abstinence-only sex education — a method largely considered an ineffective way to reduce pregnancy and rates of sexually transmitted infections among teens. A more effective method of offering pandemic health guidance might include telling people that if they aren’t able or willing to gather with others virtually, which poses the lowest risk for transmission, then they should consider the risks involved with in-person gatherings and use that knowledge to make an informed decision about how to gather.
Reaching the people who need that information, however, can be difficult as misinformation about the virus online and elsewhere abounds, Murphy-Ende said. Online communities often share messages that reinforce their own biases — including conspiracy theories and outright denial that COVID-19 poses serious health risks.
Communicating with people on an individual level could make a difference, said Ajay Sethi, an epidemiologist and associate professor in the Department of Population Health Sciences at the University of Wisconsin-Madison.
“Online you’ll see people saying, ‘You’re an idiot,’” Sethi said of how others respond to people who present misinformation. “But if someone were to say that I’m an idiot, I probably would shut down and stop listening.”
After graduating from college, Sethi said he was a crisis counselor for two years. And while misinformation isn’t akin to crisis, he said the same principles could apply to communicating with people who don’t trust the public health messaging around COVID-19.
“Eighty percent of the time, you listen,” Sethi said. “Never try to steer someone into solutions too early.”
Seth said it’s important to figure out where people are coming from, and to give them the “compass” to find the right information on their own. This allows them to feel some sense of control.
“But they have to take that first step, and that restores one’s control in a crisis situation,” Sethi said.

Wisconsin Public Radio, © Copyright 2025, Board of Regents of the University of Wisconsin System and Wisconsin Educational Communications Board.