
The patient sat in Dr. Shefaali Sharma’s exam room, distraught. She was pregnant with her third child. Just weeks earlier, the U.S. Supreme Court had revoked the federally protected, constitutional right to an abortion, restoring Wisconsin’s near-total abortion ban from the 1800s.
“I need to know how this might impact, like, labor and delivery,” the patient said, referring to the court decision. Then she trailed off: “I guess, I just …”
After a few moments, she summoned her courage.
News with a little more humanity
WPR’s “Wisconsin Today” newsletter keeps you connected to the state you love without feeling overwhelmed. No paywall. No agenda. No corporate filter.
“If it comes down to me or the baby, I need you to pick me,” she told Sharma. “I have two babies at home that I have to take care of.”
Sharma, a Madison-based obstetrician and gynecologist, assured her patient that doctors would take care of her. (Sharma does not typically perform abortions, but other physicians in her practice do.)
“She should be enjoying her last pregnancy and savoring moments with her family of four before it becomes a family of five,” says Sharma, recalling the interaction a few weeks later. “She should be enjoying these moments and not worrying whether or not she will die because of politicians making life decisions for her.”

The Supreme Court decision that overturned federal abortion rights remains unpopular. A majority of Americans and Wisconsinites oppose outlawing abortion. Public approval of the high court has plummeted since the decision was issued. And four of the five-justice majority in the Dobbs decision were appointed by candidates elevated to the presidency without winning the popular vote.
Conversations like Sharma’s echo in hospitals and doctor’s offices across Wisconsin. Physicians attempt to reassure their patients that they will receive treatment if their water breaks too early or they suffer a miscarriage — all while working with lawyers to determine the circumstances in which they can provide abortions without risking a felony.
“There is no clarity currently, and no consensus,” says Dr. Wendy Molaska, president of the Wisconsin Medical Society.
In the absence of statutory or administrative guidance from the state, professional associations, health systems and hospitals — even physicians themselves — are developing policies to guide pregnancy-related care.
The Medical Society has been working with the Wisconsin section of The American College of Obstetricians and Gynecologists, other health care entities and outside counsel to develop legal guidance on the state’s abortion laws. Molaska expects its release to physician members soon. The Wisconsin Hospital Association declined to say what, if any, guidelines it is developing.
But whatever advice they provide will not be binding — nor universally applicable. The circumstances under which a person will receive an abortion in Wisconsin will ultimately depend on the health system or hospital — and, when it comes down to it, individual doctors. Even then, the approach will vary case by case.
“Ultimately, the physician(s) actually signing off on or performing the procedure will be responsible for defending its necessity,” says Richie Davis, an attorney with Quarles and Brady, in an email to Wisconsin Watch. The firm has advised Wisconsin health systems and physicians on how to provide care without violating the law. “Liability will turn on the facts and circumstances surrounding the specific patient.”

Adds John Eich, director of the Wisconsin Office of Rural Health, part of the University of Wisconsin School of Medicine and Public Health: “It’s going to be some line in between patient needs and legal risk, and each system will likely have to weigh several in-house factors to draw it.”
And any guidelines developed by a health system, hospital or professional association will likely provide broad principles in lieu of specific conditions.
“It’s really important to understand there’s never going to be like a checklist,” says Dr. Lisa Barroilhet, a gynecologic oncologist and the interim chair of obstetrics and gynecology for the UW. “Even before there were particular concerns about the legal ramifications, these situations are always incredibly individualized and nuanced.”
Beyond the variability, some physicians fear that codifying a list of situations in which an abortion is legal will open them up to prosecution anytime they perform one in a situation that’s not spelled out in the guidance.
‘Ambiguous’ wording creates confusion
Wisconsin’s ban makes providing an abortion in almost all cases a Class H felony, punishable by up to six years in prison and a $10,000 fine. Physicians convicted of a felony might also lose their medical licenses, rendering them unable to practice. The statute of limitations for most felonies is six years.
“The Wisconsin law is rather ambiguous, and a reasonable clinical disagreement on medical necessity can expose a physician to potential criminal liability,” Davis says. “Even if a physician can win at trial and avoid criminal liability, that same physician may be arrested, detained with a high bail, suffer public shame and effectively have their practice destroyed for performing an abortion which they believed was medically necessary to save the life of the mother.”
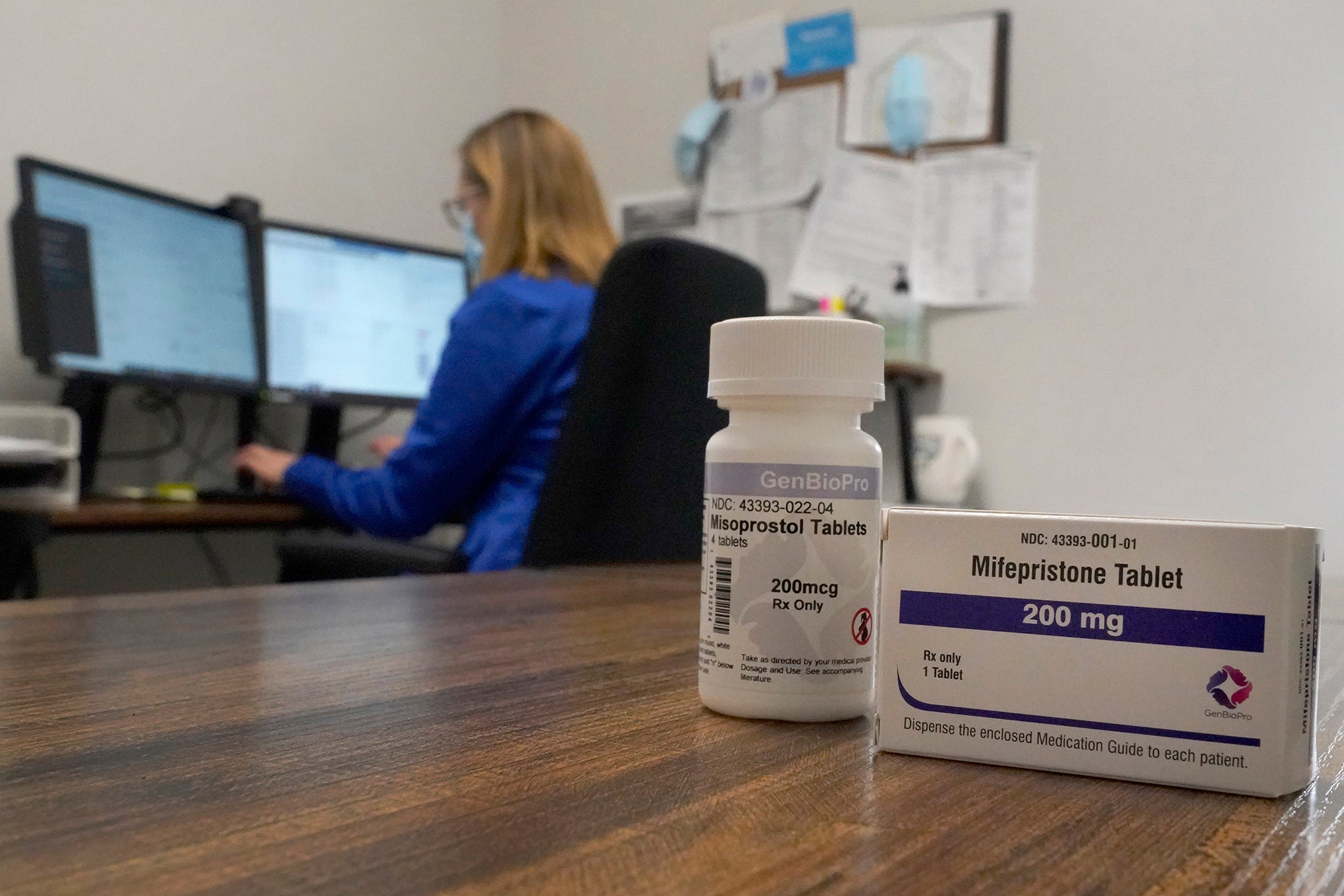
The law contains one exception, a “therapeutic abortion” — which physicians say is an archaic term. The law says the procedure must be deemed necessary “or is advised by 2 other physicians as necessary, to save the life of the mother.”
The statute defines abortion as the intentional killing of an “unborn child” — defined as an embryo or fetus “from the time of conception until it is born alive.”
“Unlike other states which center on the presence of a ‘fetal heartbeat’ to determine whether a fetus is protected under an abortion law, (Wisconsin’s abortion law) casts a wider net,” writes Davis.
But he says the law turns on intent. Any prosecutor who criminally charges a physician must convince a jury — or compile sufficient evidence to secure a plea deal — that the doctor knew the medical procedure would terminate the pregnancy, had no reasonable basis to believe the procedure was necessary to save the mother’s life and did it anyway.
“Negligent or reckless actions will not suffice,” Davis says.

Molaska considers the statute outdated, vague — and severe.
Outdated because Wisconsin’s law predates even foundational tenets of modern medicine such as germ theory. Vague because unlike Texas, Wisconsin does not spell out exceptions for ectopic pregnancies or removal of a fetus that has already died. Severe because unlike Alabama, Wisconsin does not allow intervention to “prevent a serious health risk” — only to save a pregnant person’s life.
Molaska says this leaves doctors “between a rock and a hard place.” She asks, “Where’s the line that I let her get sick enough so that her life is in danger?” Or, she wonders, would a physician be barred from removing a deceased fetus if the body does not pass it?
In practice, that degree of interpretation, and the likelihood a physician will face arrest and prosecution for providing a life-saving abortion, will depend on the zealousness of local law enforcement and prosecutors. For example, Sheboygan County’s district attorney, Republican Joel Urmanski, told TMJ4 he would press charges if he found probable cause that an alleged abortion violated state law. The Democratic chief prosecutors in Dane and Milwaukee counties have announced they will not investigate abortions.
These “gray situations” will have “‘black and white’ effects” on patients, Wisconsin physicians said in a press call.
After Texas passed its six-week abortion ban, research by Parkland Health and UT Southwestern Medical Center found that, compared to patients in states allowing immediate abortions, delayed treatment nearly doubled the incidence of serious health complications.
‘Uncertainty’ in Wisconsin over care
Approaches to care in Wisconsin will vary until lawmakers or judges resolve the question of when an abortion becomes life-saving and therefore legally permissible.
Wisconsin Watch attempted to contact 48 hospitals or health systems across the state through email and phone calls. Many did not respond. A few provided brief statements in lieu of answers to questions.
The Richland Hospital and Clinics, for example, wrote that its staff wanted to “reassure patients” that its care “has not changed. Our services like pregnancy care and miscarriage management are not impacted.” Any concerned patients should contact their health provider.
Meanwhile, the Froedtert and Medical College of Wisconsin health network said in an email that it is “still analyzing the recent Supreme Court decision, which creates some uncertainty in Wisconsin.”
Tomah Health said it provides care per the Emergency Medical Treatment and Labor Act, or EMTALA. The 36-year-old federal law applies to all hospitals with emergency services that receive Medicare funding, requiring staff to provide stabilizing treatment to patients in emergency situations.
Last month, following an executive order from President Biden, the U.S. Department of Health and Human Services released guidance reinforcing that the law preempts any state-level abortion ban, requiring physicians to provide an abortion if a patient is “experiencing an emergency medical condition as defined by EMTALA, and that abortion is the stabilizing treatment necessary to resolve that condition.”
In early August, the U.S. Department of Justice sued Idaho over its near-total abortion ban. Like Wisconsin’s, Idaho’s law permits abortions to save patient’s life — but not to help the patient avoid severe health consequences, such as permanent disability. The lawsuit alleges Idaho’s law violates EMTALA.
One Wisconsin physician, requesting anonymity because of lack of authorization to speak to the media, says some doctors have established their own approaches. That physician says from the perspective of their hospital — which even prior to the Dobbs decision only performed abortions in life-saving circumstances — the circumstances had not changed. Only the physician — not the health care facility — faces arrest, prosecution or incarceration, the doctor noted.
Consensus on ‘life-threatening’ ectopic pregnancies
The OB-GYNs interviewed by Wisconsin Watch outlined a few clear cases in which they would provide abortions, and they expressed frustration at the vast array of murkier instances.
After an initial period of uncertainty, Dr. Kristin Lyerly of Green Bay and Dr. Sarah Goetz of Marshfield determined they would treat ectopic pregnancies without disruption. Lyerly, who previously ran for Wisconsin state Assembly and holds a regional leadership role with The American College of Obstetricians and Gynecologists, notes that these circumstances never required the same paperwork as other abortions.

“So we personally are going to support each other and treat ectopic pregnancies when they present,” she says. “Ectopic pregnancies are life-threatening. They’re the number one reason that women die in early pregnancy.”
The American College of Obstetricians and Gynecologists distinguishes this treatment from other forms of abortion care. “A tubal ectopic can never be a viable pregnancy, so it is generally viewed outside of abortion,” says Kate Connors, a spokesperson, by email.
Davis, the attorney for Quarles and Brady, agrees it’s “reasonable to rely on the ‘therapeutic abortion’ exception” to remove ectopic pregnancies, and physicians may not need to wait.
UW Health’s Barroilhet says her legal team has broadly distinguished between pregnancies that can and cannot result in a live birth. When it comes to ectopic pregnancies or miscarriages in which the fetus has died, patients will get standard care — medication or surgical procedures — without the patient experiencing much, if any, change.
Sharma, the Madison-based OB-GYN, agrees. She has told her patients that “relatively speaking, they won’t see a big change in management” and care for miscarriages.
“However, on our end, we’re just doing some increased documentation to confirm and demonstrate that it was a non-viable pregnancy and perhaps having an additional ultrasound at a certain interval to provide objective data,” she says.
Other situations remain murky
But these two examples belong to just a handful of clear-cut situations a physician can predict.
If a person’s water breaks before the fetus is viable, or if the patient is hemorrhaging but the fetus still has some detectable cardiac activity, the approach is less clear.
“Now we’re getting into the very nuanced, individualized situations where there may be situations that are life-saving indications and there may not be,” Barroilhet says. “And you really have to look at the patient in front of you, and all the specifics of that situation to make the best decision and, of course, the patient’s wishes factoring heavily into that.”
Mere days after the Dobbs ruling, Goetz, the Marshfield doctor, received a call from a doctor at a satellite center. The patient had her water break at 17 weeks; normal gestation is 40 weeks, and viability is considered to begin at 24. The doctor was “a little at a loss” of what he could offer her, Goetz says.
She recalls telling her colleague that she believed the law prevented them from offering to induce labor.
Later, the patient went into labor naturally, delivering the pre-viable fetus on her own.
“But that’s one of the types of cases that we’re most concerned about as a group,” Goetz says.
Physicians are particularly concerned because otherwise young, healthy patients can decline rapidly, leaving mere minutes to provide life-saving treatment.
If a patient starts to miscarry, but she and her colleagues can still detect embryonic or fetal cardiac activity, they plan to legally protect themselves by having three physicians document how an abortion is necessary to save the person’s life.
“Our ability to use clinical judgment and data is going to be severely restricted,” Sharma says. “There will be some delays in care.”

No changes at Catholic hospitals
For physicians in Wisconsin’s Catholic hospitals, the Dobbs ruling changed nothing.
Catholic hospitals, which comprise about one-third of all hospitals in the state, did not perform elective abortions prior to the court decision.
But Dr. James Linn, an OB-GYN at Ascension and a member of the American Association of Pro-Life Obstetricians and Gynecologists, says he and his colleagues have and will continue to provide life-saving treatment for ectopic pregnancies and miscarriages, the latter of which are “very common.”
“About an hour ago, I was taking care of a miscarriage at the hospital where I work,” says Linn, who says he performed a suction dilation and curettage to remove a fetus who had died in utero. “It was the same procedure that’s done at abortion clinics all over the country… So those things are still routinely done.”
If a pregnant patient’s water broke too early and they began to show signs of infection, he says he would provide antibiotics and “separate the mother from the baby” by inducing labor — even if the health is not at risk.
Brian Reardon, spokesperson for the Catholic Health Association of the United States wrote by email: “In tragic situations when the mother suffers from an urgent, life-threatening condition during pregnancy, Catholic health clinicians provide all medically indicated treatment even if it poses a threat to the unborn child or may result in the unintended death of the child.” He cited examples of ectopic pregnancies and uterine infections, saying, “Such procedures are both clinically and ethically required.”
For Linn, as with Wisconsin’s abortion statute, intent matters. He considers an abortion “a procedure where the intent is to end the life of a human being in the womb.” In these cases, “your intention is not to cause the death of a living, human being. Your intention is to try to save them both.”
He says concerns over physicians’ abilities to save pregnant patients’ lives by terminating pregnancies is “misinformation” that is “being used politically to rile people up to get, you know, get votes.”
To physicians who must use the life-saving standard for abortion care that those at Catholic hospitals have used for years, he says: “Just be honest.”
“If you think your (patient’s) life is at risk from continuing this pregnancy, you do the right thing,” he says. “If you’re being honest, and you’re an expert, I think you’ll get the benefit of the doubt from the court.”
Delays loom in rural areas
But some physicians say delays and potential danger may be elevated — particularly in rural parts of the state. It may be harder for doctors to find two other physicians to sign onto a procedure — although Goetz, in Marshfield, says she’s made contact with her colleagues across the state to facilitate this.
And while rural emergency departments may have sufficient equipment and resources to intervene while a patient is stable, they might not have enough blood or may not be able to transfer the patient elsewhere in time to save a life, Molaska says.
“Because of staffing issues,” she says, “if you’re up in northern Wisconsin, good luck getting that patient to a higher level of care quickly enough.”
She worries about nonviable pregnancies that can turn life-threatening if left untreated.
“Can I intervene now, knowing what I know, that this woman’s life will eventually be in danger, and risk a felony?” Molaska asks. “Do we have to wait for that woman to become septic so that we can get her abortion even though there’s no living fetus?”
“I think it’s just really hard right now because there’s so many of these different gray situations, and the law tends to be more black and white. It doesn’t account for any of these currently.”
The nonprofit Wisconsin Watch (www.WisconsinWatch.org) collaborates with WPR, PBS Wisconsin, other news media and the University of Wisconsin-Madison School of Journalism and Mass Communication. All works created, published, posted or disseminated by Wisconsin Watch do not necessarily reflect the views or opinions of UW-Madison or any of its affiliates.